Response to chemotherapy of immunohistochemical phenotypes of breast cancer patients.3
Phenotypes markers expression and Phenotypes distribution:
141 tumors were available for CK 7/8, 18 and 19, CK5/6, 14 and SMA analyses respectively. A very high proportion of cases, 65.2%, demonstrated positivity for the luminal cytokeratins 7/8, 18 and 19. In contrast, a lower proportion, 9.9%, showed expression of the basal markers. There was a highly significant inverse correlation between the luminal (CK 7/8, CK18 and CK19) and the basal (CK 5/6, CK14 and SMA) immunoprofiles (p < 0.05).
We found that expression of luminal markers was associated with good prognostic tumour characteristics: 62 patients were grade 1 and 52 patients had only one to three lymph nodes affected. These findings are in contrast to the expression of basal markers, which was associated with poor prognostic features: 17 patients had more than 10 lymph nodes affected and 15 patients were grade 3, both of them were statistical significant (p<0.05).
Luminal phenotype was present in 65.2% of the cases, basal phenotype in 9.9% and HER-2 phenotype in 8.5%. In 16.3% of the tumors the phenotype were considered null/no expression.
Phenotypes and survival.
Median DFS for basal phenotype was 24 months, and for luminal and HER-2 phenotypes the median disease DFS was not reached. Five years disease free survival was as follows: basal phenotype 19%, luminal phenotype 63% and HER-2 56%. The DFS analysis by phenotypes subtypes has not been reached statistical significance. Nevertheless, when the same analysis for basal phenotype compared with non basal phenotype was done, the difference was highly significant showing that the presence of a detectable basal phenotype was associated with a worse disease free survival (Figure 8) (p= 0.0001).
Figure 8. Disease free survival (months).

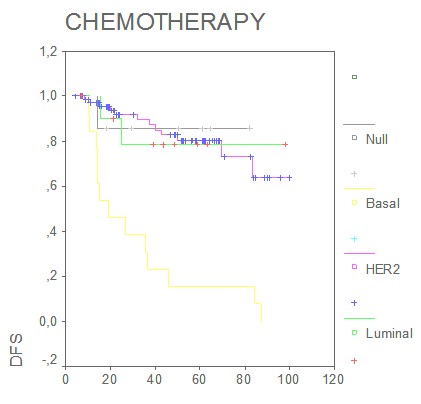
Interestingly, multivariate Cox regression analyses estimated that the prognostic effect of basal phenotype in relation to disease free survival was independent of lymph node, stage and tumor size (HR 0.12; 95% CI 0.05-0.2; p<0.05) The analysis of the possible predictive value of tumor phenotypes found that in the group of patients who received standard-based adjuvant chemotherapy, DFS was significantly shorter in the basal phenotype, (p= 0.001) (Figure 9, months).
Figure 9:
Discussion
In the last few years the studies of gene expression patterns or inmonohistochemical profiles focusing in breast cancer (43,44,45,46,47), have been shown that is possible to predict the behavior of the disease more accurately than by classical prognostic factors only.
Recent cDNA gene expression analysis and immunohistochemical studies have proposed two distinguishable groups with luminal and basal phenotypes that have different cytogenetic alterations and protein expression patterns (22,23,36,37,39,40)
Our results demonstrate on a well-characterized and followed series of primary breast cancer that a high proportion of 65.2% invasive breast carcinomas express only the luminal epithelial cell cytokeratins and have a pure luminal cell phenotype. Exclusive expression of the basal epithelial markers was restricted to a very small subset. Previous studies have also recorded that the luminal CKs 7, 8, 18 and 19 are predominantly expressed in breast cancer (15), like in our study. Expression of the basal markers CK 5/6, CK14 and SMA has been reported in invasive breast carcinoma, ranging from 4% to 16% of cases (16). This is in agreement with our study, wherein the expression of the basal phenotype was positive in 9.9% of the cases.
On studying the association between the expression of these markers with different clinical and pathological parameters, we found that expression of luminal markers were associated with good prognostic tumor characteristics and outcome, in contrast to the expression of basal markers, which was associated with poor prognostic features and behavior. These findings are in accordance with previous studies where an inverse association between CK 8, 18 expression and tumor grade, recurrence rate and estrogen receptors negative status has been reported (17, 43). They also support previous data which have shown that highly metastatic cell lines are associated with loss of CK 18 expression (18).
In our series the presence of a detectable basal phenotype was highly significantly associated with a worse prognosis, so that the DFS at 5 years were nearly three times greater in the non basal group than in the basal one.Similar results have been reported by other authors. Perou et al (23) found that women with basal-like breast cancers had shorter relapse-free survival times than women with other types of breast cancer. Basal-like breast cancers also have a tendency toward visceral (versus bone) metastasis (24). In an analysis of 49 patients with basal-like breast cancer and 49 matched controls, Banerjee et al. (25) found that patients with basal-like breast cancer had significantly shorter disease free and overall survival times than women with other tumors, but basal-like status was not a significant independent prognostic variable in the multivariable analysis.
Studies on patients with basal-like breast cancers have been limited by small sample sizes and short follow-up times. To some extent, this is due to the basal-like phenotype is based on immunohistochemical staining of tumor slides using anti-keratin antibodies, and these are not yet in general clinical use. However, the ‘‘basal-like’’ category of tumors is composed almost entirely of ‘‘triple-negative’’ breast cancers [i.e., tumors that are negative for estrogen receptors, progesterone receptors (PR), and HER2]. It is therefore possible to classify with accuracy the majority of basal-like breast cancers (and non– basal-like breast cancers) using these three standard immunohistochemical markers. Dent et al published very recently (26) a large series of triple-negative breast cancers derived from a single institution with long-term follow-up. They were able to show that the triple-negative category of breast cancers exhibits a distinct pattern of recurrence. This pattern is characterized by a rapidly rising rate in the first 2 years following diagnosis, a peak at 2 to 3 years followed by a decline in recurrence risk over the next 5 years, and a very low risk of recurrence thereafter. Unlike women with other types of breast cancers, the great majority of women with triple-negative cancers who had no evidence of progression after 8 years did not recur thereafter.
Expression of the luminal markers was significantly related to longer DFS in our series, in particular, patients with high or moderate expression showed better DFS than those cases with low or no expression of these luminal markers. The converse was observed in tumors that labeled with the basal markers, where positive cases were associated with poor outcome particularly with CK 5/6 expression, which proved to be an independent prognostic predictor for DFS. Previous studies have reported that CK 8 is associated with better overall survival and is an independent prognostic indicator of DFS, and that CK 18 expression is an independent prognostic factor in predicting DFS In contrast, a significant association has been reported between poor overall survival and expression of the basal markers, CK 5/6 and 17, and these markers also had an independent prognostic impact in patients without nodal metastasis. Positivity for both CK 5/6 and SMA was reciprocally related to age, supporting the finding that breast cancer in younger women is more aggressive, with lower hormone receptor levels, higher proliferation and a worse prognosis compared with those in women of older age (19).